Genicular Artery Embolization for Knee Pain: A Non-Surgical Path Forward
-
March 15, 2026
- Posted by: Nina Rand
For many people living with knee osteoarthritis (OA), every step is a reminder of how much the condition affects daily life. Whether it manifests as difficulty climbing stairs, reduced independence, or simply the chronic ache that makes a good night’s sleep feel impossible, knee OA is more than a nuisance—it severely reduces quality of life.
What makes treatment decisions even more complex is when a patient is also managing cardiovascular disease, taking blood thinners, or carrying other health conditions that make traditional joint replacement surgery a serious concern. For these individuals, the gap between conservative options like injections and major surgery can feel frustratingly wide.
Genicular artery embolization (GAE) is an interventional cardiology procedure that may offer a meaningful path forward for appropriately selected patients. It is minimally invasive, performed on an outpatient basis, and targets the underlying cause of pain, making it a particularly relevant option for those who cannot safely pursue or wish to delay surgical intervention.
For our patients in Houston and across the Gulf Coast region, access to interventional cardiology expertise continues to grow, expanding who can realistically benefit from this type of care.
Understanding Genicular Artery Embolization and How It Works
 Genicular artery embolization is a minimally invasive procedure performed by an interventional cardiologist that targets the vascular changes that drive chronic knee pain in osteoarthritis.
Genicular artery embolization is a minimally invasive procedure performed by an interventional cardiologist that targets the vascular changes that drive chronic knee pain in osteoarthritis.
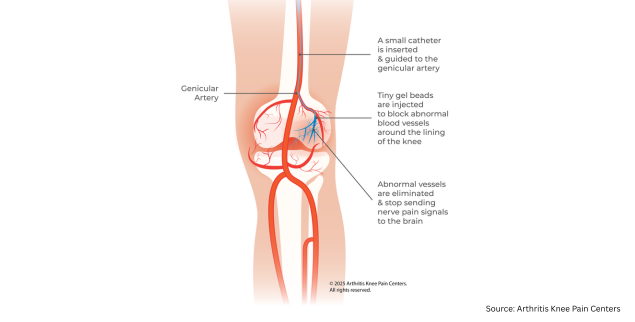
In a healthy knee, blood flow is well-regulated. But in osteoarthritic joints, chronic inflammation triggers the growth of abnormal new blood vessels in the synovium, the tissue lining inside the knee joint. Think of the synovium like a cushioning layer that, when inflamed, becomes flooded with tiny blood vessels that deliver pain signals to the joint. This process is called angiogenesis. And the result is persistent pain that can be difficult to control through conventional means.
GAE works by carefully reducing that abnormal blood flow. Using real-time X-ray imaging (called angiography) for guidance, the interventional cardiologist threads a very thin, flexible tube—called a microcatheter—through the arteries to reach the blood vessels supplying the inflamed knee lining. Tiny particles are then released through the tube to partially block those vessels, which reduces inflammation and, over time, knee pain.
The procedure is performed entirely on an outpatient basis under local anesthesia. There is no surgical incision, no general anesthesia, and typically no hospital stay. Most patients go home the same day.
Why Patients with Heart Concerns May Consider GAE

Knee replacement surgery is a major orthopedic procedure that carries well-established perioperative risks. For patients with cardiovascular disease, these risks are amplified. General or spinal anesthesia, significant blood loss, prolonged immobility, and the physiological stress of surgery create a risk profile that may make joint replacement inadvisable or, at minimum, something to defer as long as possible.
Patients on anticoagulation therapy face additional challenges. Discontinuing blood thinners before surgery introduces thromboembolic risk, while continuing them elevates the risk of bleeding complications. Bridging protocols are complex and not without hazard.
For referring physicians managing these patients, GAE offers a relevant alternative. As a non-surgical knee pain treatment, it carries a fundamentally different risk profile than joint replacement:
- Performed under local anesthesia, avoiding the systemic stress of general or regional anesthesia
- Minimal blood loss compared to orthopedic surgery
- No requirement for extended anticoagulation modification in most cases (though this should be evaluated on an individual case-by-case basis)
- Faster recovery with less overall physiological burden
- Outpatient procedure with same-day discharge in most cases
While GAE is not appropriate for every patient, it deserves a place in the conversation—especially for those with significant comorbidities who are caught between inadequate conservative care and high surgical risk.
Who Is a Candidate for Genicular Artery Embolization?
Not everyone with knee pain will be a good fit for GAE. The goal is to match the right procedure to the right patient. Here’s a breakdown of who tends to benefit most and who may need a different approach.
GAE may be a good option if you:
- Have mild to moderate knee arthritis
- Still have significant pain despite trying physical therapy, anti-inflammatory medications, or injections (such as cortisone or gel injections)
- Are not ready for knee replacement surgery, or prefer to delay it
- Have health conditions—like heart disease, diabetes, or obesity—that make surgery higher risk than average
GAE may not be appropriate if you:
- Have severe, end-stage arthritis where the joint is significantly worn down. At that point, structural repair through joint replacement is usually the better path
- Have an active infection in or around the knee
- Have blood vessel problems that would make the catheter-based approach unsafe
To find out if GAE is right for you, our team will review your knee imaging (X-rays and possibly an MRI) and your full medical history. For patients with complex health conditions, such as a history of heart disease or blood-clotting concerns, an interventional cardiologist from Texas Cardiology Associates will work closely with your cardiologist or primary care physician to ensure the evaluation is thorough and the plan is safe.
What to Expect Before, During, and After the GAE Knee Procedure
 Before the Procedure
Before the Procedure
Your journey begins with a thorough consultation and imaging workup. Your care team will review your knee X-rays and may order an MRI to get a clearer picture of the arthritis and the surrounding tissue. Your medications (including any blood thinners), heart health, and overall medical history will all factor into whether GAE is the right choice for you and how to proceed safely to ensure you’re set up for the safest possible experience.
During the Procedure
The procedure typically takes one to two hours. You’ll be awake the whole time—no general anesthesia required. After numbing the skin at the access point (usually the wrist or groin), the interventional cardiologist uses real-time imaging to guide a tiny, flexible tube into the blood vessels around your knee. Once in the right position, small particles are released to reduce blood flow to the inflamed tissue. Most patients typically report little to no discomfort during the procedure and are able to talk with the team throughout.
After the Procedure
Some soreness around the knee in the first few days is normal and usually manageable with over-the-counter pain relievers. Most patients are up and moving with light activity within a day or two. Pain relief tends to be gradual—many people start to notice a real difference four to eight weeks after the procedure as the inflammation settles.
Follow-up appointments are important for tracking how you’re responding. It’s worth setting realistic expectations: GAE eases pain and improves knee function, but it doesn’t reverse the underlying arthritis or repair joint damage. For many patients, that level of relief is still significant and life-changing. Research also shows that for most patients, results hold up well over one to two years, with only a small percentage needing a repeat procedure or eventually moving on to knee replacement.
Risks and Side Effects of GAE for Knee Osteoarthritis
Risks and Side Effects
GAE has a favorable safety profile. The most commonly reported side effect is temporary skin discoloration near the knee, occurring in approximately 11.6% of patients and typically resolving on its own (pmc.ncbi.nlm.nih.gov). Minor bruising at the access site is also common. A small number of patients experience brief numbness or tingling in the area, which usually resolves within two weeks. Serious complications are rare and are further minimized by careful pre-procedural planning and the interventional cardiologist’s experience.
Taking the Next Step
If you or someone you know is living with chronic knee pain and facing limitations due to cardiovascular risk, blood thinner use, or other health conditions, genicular artery embolization may be a conversation worth having. No single treatment is right for everyone, and the best outcomes come from a personalized, multidisciplinary approach to evaluation.
Connecting with a specialist in interventional cardiology—ideally in coordination with your primary care physician—is the best first step toward understanding whether GAE is right for you. An open conversation about your goals, imaging, and medical history can help your care team determine whether this emerging option is appropriate for your treatment plan.
We welcome referrals and consultations for patients who may benefit from GAE for knee pain. If you have a patient who might be a candidate for the GAE knee procedure, or if you’d like to learn more about it, please reach out to our team.
Frequently Asked Questions About Genicular Artery Embolization (GAE)
Does GAE really work for knee pain?
Clinical studies show that most appropriately selected patients experience meaningful pain reduction following GAE. Results build gradually over four to eight weeks, and improvements have been shown to last for 12 and 24 months (evtoday.com). That said, results vary from person to person, and GAE works best for patients with mild to moderate arthritis who haven’t gotten enough relief from earlier treatments.
What are the disadvantages of genicular artery embolization?
GAE does not repair or reverse structural joint damage, so it isn’t the right choice for patients with end-stage arthritis. It also costs more than repeat injections, and while the early research is promising, the evidence base is still building. Temporary side effects such as skin discoloration are relatively common, and a small number of patients may need a repeat procedure or eventually undergo knee replacement.
Is genicular artery embolization better than knee replacement?
These procedures serve different patient populations and goals. Knee replacement offers a definitive solution for surgical candidates with end-stage OA. GAE offers a less invasive option for those with mild to moderate OA or significant comorbidities. For many patients, the two procedures are not directly comparable because joint replacement may not be safe for them.
Who can have genicular artery embolization?
Good candidates are generally people with mild to moderate knee arthritis who still have significant pain despite conservative treatments, and who are either not ready for or not able to have knee replacement surgery. Patients with heart disease, blood-clotting conditions, diabetes, or other health concerns that increase surgical risk are often the most appropriate candidates. A full evaluation, including imaging and a review of your health history, is needed to confirm whether GAE is right for you.
Are there any risks associated with GAE?
GAE has a strong safety profile overall. The most common side effect is temporary skin discoloration near the knee, affecting roughly 1 in 10 patients and resolving on its own. Some patients experience minor bruising at the access site or brief tingling, both of which are temporary. Serious complications are uncommon. As with any procedure involving catheters and contrast dye, there are small risks that your care team will review with you in detail before you proceed.